
Hypochondriac, Conversion Disorder, Anxiety, Depression all things people with rare disorders or unusual presentation are bound to be told they have at some point. True our horrible symptoms can casue psychiatric complications. Who wouldn’t be anxious when your joints suddenly dislocate or you vomit at random and people keep telling you its all in your head? That doesn’t mean we don’t have a very real physical cause for our symptoms.
Its seems the medical motto for I have no clue whats wrong for you and don’t care to look is “when in doubt psych it out”. If they cant see it on an x-ray or blood test its whole lot less effort and frustration to turf a patient to psychiatric care. That doesn’t make it acceptable or ok. Though it happens with many illnesses as May is Ehlers Danlos Syndrome (EDS) awareness month lets pull that to the forefront.
The following are a list of conditions often misdiagnosed as psychiatric that are firmly physical and have a higher comorbidity in people with EDS.
Aneurysm – Primarily a feature of vascular type but possible to present in others is an increased risk for aneurysm. Symptoms vary depending on the location of the defect but can include headache, stiff neck, abdominal pain, nausea, and fatigue. Before the aneurysm protrudes into other structures or ruptures these symptoms can be significantly less severe than we are lead to believe. Therefore they can end up explained away by more common conditions such as stress related high blood pressure.
Anesthetic/Analgesic Issues – Though not fully understood in medical literature it is common for people with EDS to process both anesthetics (numbing agents) and analgesics (pain killers) differently. We tend to metabolize them faster than the general population e.g. Novocaine at the dentist. We are also prone to more severe side effects from analgesics.
For instance on the occasions I need an outpatient procedure or pain management in hospital I choose Fentanyl a synthetic opiate fifty times stronger than Morphine not due to its potency but that it has proven in my case to have less adverse effects. If they choose not to accommodate that request I will deny pain medication as I have found its not worth the short or longer term adverse reactions. What good is Morphine if I end up back in the hospital three days later from an intestinal obstruction that leads to use of more Morphine therefore repeating the cycle? Or using a less effective drug that still produces adverse effects? No thank you.
Each person reacts differently and may not tolerate Fentanyl as well as I do but it should be known that we are not drug seekers merely because we know our bodies better than doctors do! We are not addicts, we are not wimps, we have a biological difference in how these drugs affect us. No one should be suffering through untreated pain and no one should be referred out to a therapist and denied treatment due to that difference. In all honesty we probably need a therapist for how doctors treat us more than how our bodies behave.
Chiari Malformation – A condition that can be congenital or acquired where the brain sinks into the outlet of the skull at the top of the spine. Symptoms include headaches, visual disturbances such as blurred vision, dizziness, tinnitus, difficulty swallowing, palpitations, tingling in extremities, loss of bladder control, and sleep issues.
Many of the symptoms such as blurred vision, dizziness, difficulty swallowing, and palpitations are dismissed as anxiety. Others such as headaches, tingling, and sleep issues as ordinary stress reactions. Minimal to no testing is typically performed allowing symptoms to continually deteriorate which can resulting in loss of function, work, and eventually in some cases muscle tone and nutrition. All the while the patient being told to seek counseling and psychiatric drugs to resolve their “issues”.
Costochondritis – Is a condition in which the cartilage connecting the front ribs to the sternum becomes inflamed causing crushing pain and tightness of the chest resembling a heart attack. There is very little treatment available mainly pain management while you wait for the inflammation to pass.
Often when heart symptoms are present the course of testing are blood labs and an electrocardiogram (EKG). When blood test reveal no markers of imminent heart issues such as troponin, CK or CK–MB , serum myoglobin, and the EKG shows no noticeable electrical and rhythm changes the patient is deemed a psychiatric case and discharged without further evaluation or pain management.
Craniocervical Instability (CCI)– A condition than can occur for many reasons from injury to our natural tissue laxity. The inherent laxity involved in EDS predisposes people with EDS to inappropriate moment of the cervical spine. Symptoms may include neck pain, headaches, dysphagia, neuropathy, autonomic dysfunction including tachycardia and fainting, nausea, blurred vision, and vertigo.
Many of these symptoms are often attributed to stress and stress induced sleeping issues. As CCI can occur without any injury doctors rarely venture into further evaluation and recommend lifestyle changes to reduce stress. Not a terribly effective approach when the bones of your neck are like the end of a game of Jenga.
Cyclic Vomiting Syndrome (CVS) – Another disorder of unknown etiology that can be lifelong or periodic is CVS. Characterized by recurrent rapid onset intractable vomiting and nausea that can include abdominal pain, headache, and diarrhea. As it can be random or triggered by seemingly unrelated events (I know of a person who’s first event was triggered by riding a roller-coaster) doctors are prone to pass it off as a case of food poisoning at first occurrence and an eating disorder thereafter. How they can fathom that person living in fear of these sudden violent attacks would be the one causing them is beyond reprehensible.
Disautonomia – A broad category encompassing a variety of autonomic nervous system malfunctions such as Postural Orthostatic Tachycardia Syndrome (POTS), Reflex Sympathetic Dystrophy (AKA Complex Regional Pain Syndrome), and Syncope. Each condition presents with its unique variety of symptoms but some common ones include tachycardia, rapid change in heart rate, fainting, dizziness, nausea, visual disturbances, unexplained pain, exercise intolerance, and trouble concentrating.
Some of these symptoms are incorrectly attributed to laziness or lack of physical conditioning such as exercise intolerance, fainting, and unexplained pain. While others are seen as stress related issues. Without appropriate referrals and testing this leaves patients struggling and doctors discharging them from care for “lack of compliance” in managing weight or stress.
Gastroparesis – A motility disorder in which the stomach cannot adequately contract to digest food and expel it into the small intestine. Symptoms commonly include nausea, abdominal pain, cramping, diarrhea/constipation, new food intolerances, weight loss/gain, and fatigue.
Symptoms such as nausea, cramping, and diarrhea are typically characterized as stress related. With constipation, food intolerances, and changes in weight being misinterpreted as signs of an eating disorder. In either case they are seen as lifestyle or psychiatric issues not a mechanical disorder.
Hernia – While hernias are a fairly common condition in the general population those with EDS are more likely to experience them due to tissue laxity. A special consideration of hernias in EDS patients is that they may not present in a typical fashion in typical areas. For instance with a ventral (abdominal) hernia it may want to play “peek-a-boo” versus a more blatant or possibly strangulated hernia. If you can’t see it and don’t feel the gap in abdominal fascia due to the stretchy nature of EDS tissue how is it to be properly diagnosed? Symptoms may include nausea, feeling of a lump in the throat, and chest pain which could be inaccurately attributed to stress.
Interstitial Cystitis – A chronic bladder condition characterized by pain, burning, urgency, bloating, urinary incontinence, and frequent urination. Now I truly wish what I’m about to share didn’t happen but as someone who has interstitial cystitis and regularly speaks to others who do there are some very unfortunate rumors abound in medicine about this condition. In more than a few instances discussing quality of care and the process of diagnosis I have spoken with several people who’s doctors insisted their symptoms and pain were purely psychological and a result of repressed sexual trauma. Hows that for ludicrous “diagnosis”?
While my experience in diagnosis wasn’t good thankfully it wasn’t that terrible. This isn’t some phantom disorder with no clear cause or symptoms. Though there is debate between autoimmune and bacterial biofilm pathways there is no doubt of its existence, testing, and management. To have it dismissed as an expression of some repressed traumatic experience is a cruel disservice. Even when that is not the assumption it can still be summarily dismissed by medicine. Such as in my experience of several years of intermittent symptoms with negative urine cultures. Until I made headway in identifying the triggers and doing my own research did I get an answer that could be confirmed by doctors.
Mast Cell Disorders (MCAS/MCAD/Mastocytosis) – An atypical form of allergies in which a person has an over abundance of mast cells a type of immune cell which releases histamine and cytokines. An abundance of mast cells can lead to many symptoms such as rashes/hives, itching, flushing, nausea, vomiting, cramping, diarrhea, tachycardia, syncope, widespread pain (especially in the bones), difficulty breathing, and anaphylaxis.
Symptoms such as rashes, nausea, diarrhea, cramping, and difficulty breathing are often dismissed as stress related as mast cell attacks can be unpredictable and difficult to trace to a root cause. If they even bother looking for a cause or a severe symptom such as anaphylaxis warrants further investigation they can still come up blank. As the more definitive tests for mast cell disorders such as blood tryptase, skin biopsy, and bone marrow biopsy are rarely performed. You can have mast cell reactions linked to specific foods or chemicals and still have IgE allergy testing come up negative. Patients are often accused of being hypochondriacs, hysteric, or self inflicting rashes and other symptoms when tests to not easily uncover the true cause as mast cells.
Myofascial Pain Syndrome – A type of myalgia (muscle pain disorder) characterized by deep long lasting to permanent pain with sites called trigger points that create additional widespread pain when stimulated. As this disorder is not well understood it is rarely diagnosed or acknowledged in medicine. Though it has similarities to fibromyalgia they are in fact separate disorders. The primary difference being with fibromyalgia tender points create localized pain when stimulated whereas myofascial pain trigger points create widespread and referred pain when triggered.
Though much the same as in fibromyalgia patients with myofascial pain have an incredibly difficult journey having their pain acknowledged or treated often being accused of malingering, being lazy, or oversensitive.
Osteoporosis/Osteopenia – Another condition common in the general population with special considerations in EDS. Osteoporosis and its precursor osteopenia happen when circumstances such as age, malnutrition, medication, genetic predisposition, and genetic disorders cause thinning of the bones which leads to a brittle, porous, and fragile skeletal structure. Bones are in a constant state of re-genesis with old tissue being replaced by new. When the new tissue can no longer compensate for the loss of old structure it results in thinning bones.
The most common symptoms include easy fractures/breaks, pain, limping, stooping/poor posture, and loss of height due to collapsing vertebra. As osteoporosis is thought of an an age related condition it is often not part of the evaluation in children and adolescents. Unfortunately as has been seen in international news this can lead to drastic interference by the government in cases of suspected child abuse and neglect where none has occurred. With children being removed from their families care into custody of facilities that have no knowledge, experience, or preparation to deal with health issues the magnitude of EDS.
Even in adolescents and young adults who can advocate for themselves that no abuse has occurred it is still often not evaluated. A simple non invasive dual-energy x-ray absorptiometry (DEXA) scan can easily detect the density of the bones in multiple areas of the skeleton and confirm the diagnosis leading to appropriate intervention and care. Instead if you can navigate away from the assumption of abuse the patient is still left with unexplained pain and dismissed as having an eating disorder or malingering.
Pelvic Floor Dysfunction/Prolapse – A condition created by issues controlling the muscles of the pelvic floor affecting multiple organ systems such as the bladder, colon, and reproductive tract. Symptoms can range from constipation, feeling of inability to empty the bowel, pelvic pain, frequent urination/incontinence, and pulling/dragging sensation in the lower abdomen or pelvis.
The condition is most often associated with women who have had multiple or traumatic pregnancies. In EDS the tissue laxity doesn’t require much stress to prompt its occurrence. Whether or not EDS is diagnosed it is rarely ever evaluated in men and rarely in women under fifty who haven’t had children.
If left undiagnosed/untreated it can progress to full prolapse of organs. Prolapse is when an organ not properly supported my musculature drops either out of the body (as in rectal prolapse) or protruding down into another system (such as bladder prolapse into the vaginal canal). Up until this point it is often dismissed especially in women as “normal cycle related pains” or attributed to distention and bloating from gastric issues.
The earlier the dysfunction is diagnosed the sooner therapies can be implemented and the better the results will be. Lack of knowledge of co-morbid conditions in EDS delays this process leading to lower quality of life, increased frustration, and increased complications for the patient.
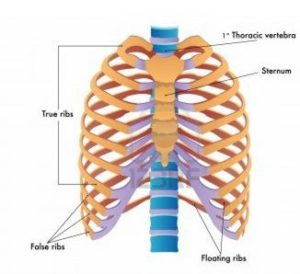
Slipped Ribs – Subluxed or dislocated ribs are a fairly frequent occurrence in those with hypermobility issues. In most cases there are no outward signs when a rib is not congruent which hinders proper diagnosis and care. Though there isn’t much to be done that can fix the issue that is no excuse to let patient live in what can be excruciating pain. Sensation and severity can vary by the patient and the location of the slipped rib(s).
Personally my worst pain is when any of the upper seven “true ribs” slip as they are more firmly anchored than the lower ribs which are mostly secured by soft cartilage as you can see in the image below. Though I do feel pain with my lower ribs its more of a deep pressure than the sharp stab of the upper ribs.
As there are no external signs slipped ribs are often dismissed, especially as people with EDS are accustomed to living in a great degree of daily pain and may not react the way doctors are trained to expect. I have never been to the ER or urgent care for a slipped rib or to have one relocated. I learned many years prior to knowing of EDS that doctors did not consider my pain valid so if I can still breathe and eat I will wait it out at home sadly many encounter this same issue.
If there was no precipitating injury or reason to suspect a break that could damage other interior structures and the patient isn’t screaming in agony there typically is no evaluation. Ive known slipped ribs to be misdiagnosed as heartburn, muscle strain, hernias, or stress related tension none of which will get you the evaluation and treatment you deserve.
Aside from relocating the rib(s) there isn’t much doctors can offer but they can provide necessary resources for prevention such as referrals for physical therapy to balance musculature as well as wraps, corsets, or braces to restrain range movement that can increase slipping.
Temporomandibular Joint Dysfunction (TMJ) – Already a condition commonly attributed to stress TMJ is a dysfunction of the temporomandibular joint which combines both hinged and sliding motions. With its diverse range of movement this joint is particularly prone to issues in those with connective tissue disorders such as EDS. Symptoms may include headache, difficult or painful chewing, clicking noise with movement, aching jaw, locked jaw (either open or closed), and a grinding sensation.
As it it already attributed to stress related issued such as grinding or clenching in the general population it can be especially difficult to receive adequate care. Though there is limited treatment available inadequate screening can prevent receiving help when options are available and most effective. Such as cases with overcrowding of teeth, inflammatory debris in the joint, damaged bone from injury or certain conditions such as arthritis are the cause of the dysfunction. Other treatment options include injections of Botox or corticosteroids (though not always well suited for EDS) and physical therapy or bite guards. Though the most common recommendations for pain control are ice, heat, and non-steroidal anti-inflammatory drugs (NSAID’s).
While that’s all well and good the lack of education of EDS and connective tissue disorders causes much harm to patients. I myself have had milder TMJ symptoms most of my life it wasn’t until an oral surgeon dismissing my concern and the information I provided for an extraction procedure did I experience long lasting serious issues. His aggressive use of a bite block while I was sedated and intubated (heart issues dictate I must have such procedures in the hospital and under sedation) left me with severe lock jaw for two months. I was unable to even fit a straw between my teeth for that time which is of great concern when you have multiple digestive disorders that predispose me to frequent vomiting that when unable to open the jaw can lead to choking and aspiration.
It also affected my post operative oral care as my stitches ripped out (due to not being properly anchored as the information I provided indicates) and it was extremely difficult to properly irrigate the surgical site when unable to open my jaw. Due to these issues to this day over a year later my gums have never healed properly and still bleed daily as well as my perpetually unstable jaw I have to reset several times a day to try to avoid locking. I still experience daily pain.
In instances such as mine many complications could be avoided if doctors were either properly educated or simply listened to the patient who is more knowledgeable on their condition than most doctors ever will be. Having our initial symptoms dismissed as stress related delays treatment that could prevent further issues. The mishandling of precautions in treatment can cause lasting damage the patient will have to deal with possibly for the rest of their life. Those with EDS don’t have the luxury of typical healing. Once our tissues have been stressed beyond the point of tolerance they will rarely ever recover the same function needed it is not “just stress”.
Thoracic Outlet Syndrome (TOS) – Is the name for a cluster of disorders which cause the blood vessels and nerves to become trapped in the space between the collarbone and the first rib (the thoracic outlet). This can be congenital (something you are born with) or caused by trauma, repetitive injury, surgery, or pregnancy.
There are three main types of TOS. Neurogenic which is a compression of the brachial plexus network of nerves, Vascular which is a compression of one or more veins and/or arteries, and Nonspecific when symptoms are present, not linked to another disorder, and cause cannot be determined.
Though it depends on type symptoms can include pain in the shoulder or neck, a throbbing lump near the collarbone, numbness and/or discoloration in the arms/hands, swelling of the arms/hands, cold arms/hands, Gilliatt-Sumner hand (a severe loss of padding at the base of the thumb), loss of grip strength, easy arm fatigue, loss of pulse in affected arm, and blood clots.
As there are minimal outward signs of TOS and the related pain is generally in the upper thoracic region it can be dismissed and tension related or caused by bad posture. Unless the patient has clear circulatory issues with visible or critical result such as loss of pulse and blood clots TOS can be easily overlooked leaving the patient to suffer the symptoms without evaluation or aid.
When dismissed as tension related it is very unlikely the patient will ever see testing such as provocation exams (designed to exacerbate symptoms), X-ray, ultrasound, CT, MRI, arteriography/venography, EMG, or nerve conduction studies. Depending upon cause and the results of such testing treatment options include physical therapy, muscle relaxers, NSAID’s, thrombolytics (to dissolve clots), anticoagulants (to prevent clots), and surgery such as to remove an extra or problematic rib.
This is by no means a comprehensive list of misdiagnosed co-morbid conditions but it is a start in raising awareness. This canary wont stop singing till doctors are educated and patients receive the care we deserve. We shouldn’t have to be responsible for bringing the diagnosis to our doctors when they have given up on us but currently that is the position many find ourselves in. I hope this list will be the beginning of better care for any who have struggled with unexplained symptoms of the conditions covered here.